Every year, the misuse of emergency medical services costs Memphis $20 million in budget shortfall. Unnecessary calls double response times when dealing with a life-or-death emergency.
A series of pilot initiatives by the Memphis Fire Department, along with public-private partners, seeks to curtail the trend by directing calls to the proper care.
“A few years ago the fire department noticed the nonemergent EMS calls were bogging down not only our system but also the hospital emergency rooms,” said Gina Sweat, Director of the Memphis Fire Department.
When the Strickland administration took office, focus was put on the problem with solutions rolling out through different pilot programs over the past year to alleviate the volume of nonemergency calls.
An innovation with potential for significant impact is the RADAR program.
“The RADAR program – Rapid Assessment Decision and Redirection – is a product of the steering committee and the conversations we were having. It’s an innovative idea that we are the only department in the country trying something like this,” said Sweat.
Up until the introduction of the RADAR pilot program three months ago, EMS was required to respond to every call – emergency or not by deploying an ambulance. Through the program, calls are now being classified on basis of emergency. If it does not rise to the level of an emergency, a RADAR car is dispatched.

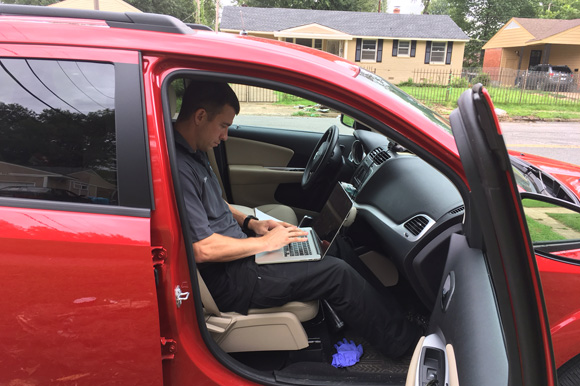
![]() Dr. Steven Euler knocks on the front door for a nonemergency call reporting nausea and dizziness.
Dr. Steven Euler knocks on the front door for a nonemergency call reporting nausea and dizziness.
“We have two RADAR cars – it’s just a little SUV – staffed with one of our paramedics and a doctor from Resurrection Health,” said Memphis Division Chief Andrew Hart.
The idea for a nonemergency vehicle came out of sidebar conversations between Chief Hart and Dr. Rick Donlon, co-founder of Resurrection Health, partners on the Community Health steering committee.
The committee was born out of a set of recommendations from an IBM grant program to foster collaboration among stakeholders in the local EMS system.
In 2015, IBM's Smart Cities Challenge awarded the fire department was awarded a $500,000 grant.
Along with the grant, IBM provided expertise and technology to address urban challenges.
Memphis was one of 16 cities out of 600 selected for the grant program.
In late February 2016, IBM’s team spent 10 days interviewing over 80 stakeholders. Principal findings centered on the 9-1-1 system. They included gaps in service, transportation, cooperation between city departments, funding, community education, to name a few.
“By the time IBM came to town, the ideas we were working on, they thought were good programs,” said Sweat. “This gave us the leverage we needed to bring in a lot of other partners to help us work on the initiatives.”
The committee, which is made of representatives from nonprofits, philanthropic organizations, hospitals, community clinics, the health department, City of Memphis and the local fire department, identified the EMS system as one of the greatest drains on city resources.
In large urban areas, like Memphis, the strain of nonemergency medical calls can be particularly acute. It often boils down to a matter of resources. Currently, there are 35 ambulances that serve the city.
While the population in Memphis has been around 650,000 since the 1970s, the coverage area EMS is responsible for has doubled in size from 170 to 350 square miles.
In 2016, EMS fielded over 130,000 medical 911 calls with 25 percent classified as nonemergent.
The high 9-1-1 call volume in Memphis is complex and based on several factors, according to the findings of the IBM team.

![]() As part of the RADAR program, paramedics carry portable equipment for checking vital signs of patients who are in nonemergency situations.
As part of the RADAR program, paramedics carry portable equipment for checking vital signs of patients who are in nonemergency situations.
A lack of transportation is one reason because calling 911 is a result of not being able to get readily access to basic care. For others, it’s not being able to pay upfront costs to see a doctor. The poverty rate in Memphis hovers around 30 percent.
“We recognize our answer for the past 50 years is if you call 9-1-1, we will give you a ride to the hospital,” Hart said.
One of the issues identified for Memphis was healthcare literacy. Many people simply don’t realize what rises to the level of an emergency. A 911 operator could just as likely field a call for a toothache as a gunshot wound.
A solution the city came up with to reduce nonemergency dispatches was to provide health care navigators for the community. These professionals help deescalate and redirect health issues that a person calling 9-1-1 may see as an emergency.
“The Health Care Navigator program was one of the first pilots that we ran. The focus was on the high utilizer group,” said Sweat.
Memphis defines a high-utilizer as a person who calls 9-1-1 four or more times in a week. In many areas of the country, one call a week is deemed high.
“We have a lot of high utilizers. When we started looking at our high utilizers, 98 to 99 percent have legitimate needs,” said Hart. “There are a variety of issues but three main ones keep coming up over and over – primary care access, transportation and behavioral/mental health.”
But these examples don’t rise to the level of an emergency. Nevertheless, an ambulance would be dispatched because another option did not yet exist.
That's where the RADAR pilot program comes in.
Any call to 9-1-1 is connected to a dispatch system. If the caller is determined to be in a nonemergency situation, then a RADAR vehicle is sent to the location.
“The advantage of sending a provider to the scene is we can make a further medical assessment doing a screening exam saying is this truly an emergency. If it is then we call an ambulance,” said Dr. Steven Euler of Resurrection Health, who is RADAR team member.
When on a call, the team will assess the patient’s situation. Paramedics will generally take vitals while the doctor consults. The doctor will then advise the patient as to the best course of action. A printed instruction is also given.
Some callers may need to go to the hospital. Others are sent to a primary care provider. The response team will call the patient’s primary care doctor and book an appointment. If they don’t have a doctor, they will connect the patient with a nonprofit. Resurrection Health, which operates three sites in Memphis, is an example.

![]() Basic equipment stored in the back seat of a RADAR car includes a stethoscope and a wireless printer.
Basic equipment stored in the back seat of a RADAR car includes a stethoscope and a wireless printer.
“We want to bolster that primary care relationship,” said Euler.
Finally, the team ensures the patient has a way to get to a doctor.
“We are finding transportation is a barrier for some folks, which is why they call 9-1-1 because they can’t get to their doctor’s office. If they call 9-1-1 then they can get a ride to the hospital,” said Euler.
But those rides are costly – about $800 a pop. They also tie up resources needed to deal with life-threatening emergencies.
Since April 10, about 500 calls have been fielded with the RADAR team. There are two teams each equipped with a car, medical equipment, doctor and paramedic. The teams work Monday through Friday, 8 a.m. to 4 p.m.
They’ve diverted about 60 percent of those calls away from the emergency room and into primary care.
Last year, 25,000 calls fell into the nonemergent category.
The doctor will be dropped from the team when the pilot ends. The longterm version of the program is still being developed. One scenario involves a team with a paramedic, trained EMT and a virtual doctor.
“Once the first responders get a set of vitals then we can FaceTime with the patient and we’ll ask a series of additional questions assess the situation,” said Euler.
If the pilot proves effective, it could be scaled up to 24 hours a day.
“Overall, going from a hundred percent (of these calls) to thirty percent needing an ambulance, that helps keeps the ambulances in service for the life-threatening emergencies. As we scale up the program, it has potential to make a big difference,” said Euler.
Starting in September, nurses will also be staffed at the EMS dispatch center. When a call in presented as nonemergent it can be directed to the nurse for further triage.
“At that point the nurse may be able to redirect them to a doctor’s visit, a clinic visit, the hospital or another right response for their need,” said Hart.
![]() At the end of a dispatch, Dr. Steven Euler records the events of the visit, including further care.
At the end of a dispatch, Dr. Steven Euler records the events of the visit, including further care.
Five part-time nurses have been hired and are in the process of training. Local hospitals will help fund the nurse pilot for a year.
Innovate Memphis has been a valuable partner in getting the EMS pilot programs running and helping them pivot to be sustainable in the long term.
“Having the expertise from Innovate Memphis has been critical to our success because even though we manage projects, it’s not our primary aspect of training. This partnership alone has kept us on track as far as the best way to manage these multiple projects we have going on,” said Hart.
Data figures prominently in EMS’ plans. As initiatives are launched, a hard-eyed assessment will be needed to gauge their effectiveness and assess where future needs lie.
“When you look at EMS in general, they, historically, have not been as research and data driven as they should be. A big piece of what they’re doing now is adding in that component,” said Hart
With assistance from Innovate Memphis, the fire department and EMS team has partnered with area colleges and outside agencies and now have actual research projects going on to study the issues so that way they will have independent, verifiable data of the programs' successes.
“We work with them to figure out how do we structure it, the resources needed, work together on grant applications, pull from the steering committee to get additional resources to test an idea and evaluate it. Then if it does work, how do we sustain it? That’s the phase we are in now,” said Justin Etzminger, director of Innovate Memphis.
While the overall focus of the pilot programs has been to alleviate the stress put on EMS, billing issues are also being addressed. Under the old system, insurers paid out only when a patient was transported to the hospital. Currently, billing codes don’t exist with insurance companies for an EMS model like the RADAR program. They will have to be created for the pilot to become permanent.
“We have been taking the data from RADAR and meeting with insurers – we are already in the contract negotiation phase. We are working on new billing codes, a payment plan for not taking people to the hospital,” said Hart.
As time goes on, expect more initiatives as the steering committee continues its work. The sustainability and expansion of the programs, which includes more RADAR cars with extended service, will figure in discussions.
“We realized there was no one fix. It was going to take several different initiatives and all of us working together to create better health care outcomes for the community,” said Sweat.